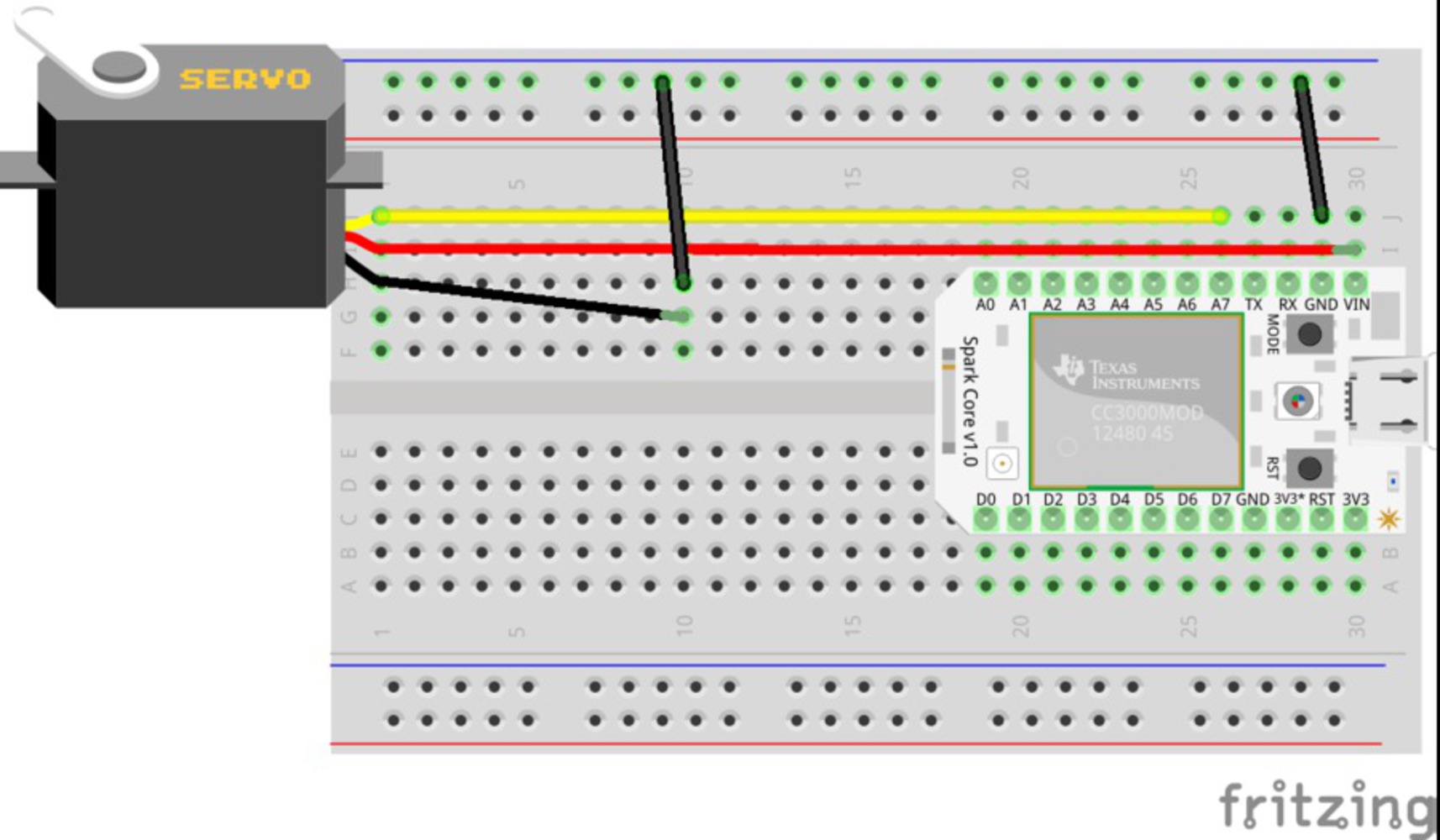
Setup
Doctors, nurses, and pharmacists can remotely monitor and control PharmaBot to write script for patients according to their body specifications, such as: body weight, height and age.
For the last 50 years, pills have been manufactured in factories and shipped to hospitals. We have now arrived at an opportunity to produce tablets much closer to the patient. Through 34 printing, the size, dose, appearance and rate of delivery of a drug can now be designed to suit an individual. The FDA has even approved one such drug already; Spritam uses 3DP technology to create a more porous pill that is easier to swallow. There are plenty of exciting applications:
-The release of a cancer-killing drug could be linked to the release of blood levels of a tumor marker. As the cancer grows, blood levels of the tumor marker would rise and this would trigger the precise release of the drug.
-Obese patients could swallow components that assemble in the stomach to create a structure that takes up a lot of room as an alternative to a gastric band.
-Some patients have to have their stomach removed as part of a treatment regimen for stomach cancer. Leveraging this technology, these patients' drugs could be designed for absorption via the intestine rather than the stomach.
The opportunities to fit the drug to the patient will increase as individuals get their own gene profile.
While the technology currently exists to modify already-made drugs via 3DP, the challenge is to digitize the chemistry in order to create encrypted blueprints for molecules, so that drugs can be built from scratch. The blueprints could be downloaded for a small fee, and the drugs can be manufactured in local pharmacies, where humans will still provide appropriate oversight, managing the process and checking the pills. With software, hardware, and chemical inks, we can drive out counterfeit drugs.
But this does not come without risk:
There is potential for blueprints to be mislabeled
There is potential for blueprints to be filed under the wrong description
There is potential for blueprints to have a higher strength than advertised
There is potential for blueprints to be hacked
We wont improve the current mechanical failure rate
And we haven't yet determined where the liability will lie when a drug causes an adverse reaction.
1. The design should be reliable. The stakes are incredibly high, and no stakeholder will embrace an unreliable design.
2. The design should be discrete and secure, satisfying HIPAA regulations.
3. The earliest phases of the design should clearly require pharmacists to manage it, while reducing risk/complexity for them, so that pharmacists will not resist it.
4. The design should be easy to use, so that pharmacists (and patients) will embrace it.
You can upload files of up to 20MB using this form.